Bruce Brodersen (right) is presented with the Veterinarian of the Year Award by Dr. Vergil Heyer
Bruce Brodersen, veterinarian, associate professor and diagnostic pathologist at the University of Nebraska–Lincoln Veterinary Diagnostic Center in the School of Veterinary Medicine and Biomedical Sciences has been named veterinarian of the year by the Nebraska Veterinary Medical Association (NVMA). Brodersen received the award at the NVMA annual convention on Jan. 21 in Kearney.
“Being a part of the NVMA has been a very enriching experience for me and the relationships that I’ve developed over the years with other practitioners has been invaluable,” said Brodersen
The veterinarian of the year award is presented annually to an NVMA member whose contributions have advanced veterinary medicine in Nebraska, and whose service has benefited the association and community.
Brodersen has been an NVMA member since 2000. He has served on the board of directors, previously held the role of association president and currently serves on the legislative and public relations committees. He was instrumental in developing the NVMA website and spearheaded Nebraska’s first Oath in Action Day sponsored by the American Veterinary Medical Foundation.
Brodersen pioneered the use of immunohistochemistry on ear notches from cattle as a means to detect persistent bovine viral diarrhea (BVD) virus infection.
“This has had a profound benefit on the control of BVD disease for bovine practitioners everywhere,” said Vergil Heyer who presented Brodersen with the award.
Working in the Veterinary Diagnostic Center since 1992, Brodersen assists veterinarians, their clients and others responsible for animal and public health in the detection, prevention and understanding of disease. He also teaches second year veterinary students in systemic pathology and public health.
New bovine export submission form
The VDC has a new submission form specifically for bovine export cases. The form is easier to complete and clarifies the ordering of tests.
Seneca Valley Virus outbreak
There has been an increase of Seneca Valley Virus (SVV), or Senecavirus A, detected in swine throughout the Midwestern United States. Although SVV has been present in the U.S. since at least the 1980s, the recent outbreak is unusual because of the number of cases observed.
Outbreaks of SVV in swine herds often result in vesicles forming on the snout and the coronary bands of the feet. These are the same clinical signs observed with foreign animal diseases such as foot and mouth disease (FMD), an economically devastating virus not present in U.S. Recent cases of SVV have also been observed with high mortality and diarrhea in neonatal (one week or less) pigs without vesicular lesions. Cases in adult swine may initially present as lameness or changes in intake.
Although SVV is not thought to pose a significant threat to overall swine or human health, it is critical that a diagnosis is made in pigs with these clinical signs so that foreign diseases, such as FMD, can be ruled out. If the clinical signs are observed, it is critical to contact your veterinarian and state/federal animal health officials.
It is not currently known how the disease is transmitted; therefore, strict biosecurity practices including control of animal and people movement should be practiced to reduce the risk of disease introduction.
The UNL Veterinary Diagnostic Center is a National Animal Health Laboratory Network (NAHLN) Lab that can test for FMD and SVV if requested by state and/or federal animal health officials as part of disease investigations.
Porcine epidemic diarrhea
By Dr. J. Dustin Loy, veterinary microbiologist, UNL VDC; and Dr. Benny Mote, swine extension specialist, UNL Animal Science Department
Porcine Epidemic Diarrhea (PED) is a disease that affects all ages of pigs and is caused by a virus (PEDV), which belongs to the Coronavirus family.
PED can, and often does, have natural mortalities approaching 100 percent in piglets less than 1 week of age; however, there are several confirmed cases where a much greater portion of neonatal piglets survive the outbreak. Those piglets along with their littermates that succumb to the virus are part of a multinational and UNL study to identify genetic markers that will explain why some piglets are able to thrive as usual on the sow, while other die. Dr. Benny Mote, swine extension specialist in the UNL Animal Science Department is involved in the study.
While most know of the high death loss in neonatal pigs, recent research has shown PEDV has detrimental effects on growth and feed efficiency of wean-to-finish pigs. This fact is often unnoticed in commercial close out sheets due to the variability in close out sheets and often the inability to separate the effect of a single disease challenge. The effect on growth and feed intake of the grower pig is distressing as most pig farms that experience a break of PEDV are finishers and are unknowingly losing production efficiencies.
The small amount of virus needed to infect a herd is as remarkable as the virus’ ability to survive long periods of time, especially in cooler/cold environments. The threat of PED outbreaks is most severe during cooler weather, and we are once again seeing an uptick in PED cases now that winter weather has arrived. Although the number of positive accessions of PEDV in Nebraska has declined each year since the 2013-14 winter, producers are encouraged to remain vigilant with internal and external farm biosecurity. A majority of the U.S. sow herd has never seen the virus due to the industry’s replacement rate. This combined with the limited immunity that follows a PED break means that the U.S. sow herd is at a much greater risk this winter than last.
PEDV is still a serious threat to the swine industry, though most likely not to the levels seen in 2013-2014. We would like to remind producers and livestock transporters to be extra vigilant with biosecurity this time of year to keep the virus out of hog farms. The UNL Veterinary Diagnostic Center offers PEDV testing, along with testing for other viruses that may clinically resemble PED, on oral fluids, feces and swabs.
Winter pinkeye
By Dr. J. Dustin Loy
Pinkeye, or infectious bovine keratoconjunctivitis, can be economically costly and a challenge to manage in affected herds. The UNL Veterinary Diagnostic Center has seen an increase in the number of submissions for winter pinkeye since fall, with some cases in feedlot cattle.
The amount of precipitation combined with delayed frost extended the normal pinkeye season and may have permitted a larger number of cases. Even in the absence of flies and insect vectors, pinkeye is highly contagious and can be spread from direct or indirect contact with infected cattle in feedyards.
Winter pinkeye is caused by the same organisms as the classic summer pinkeye. Primarily, this is the bacterium Moraxella bovis; however, a majority of cases submitted to the lab also contain Moraxella bovoculi, a closely related bacterium. The presence of other agents such as Mycoplasma bovoculi, Mycoplasma bovis or infectious bovine rhinotracheitis (IBR) can increase the risk or severity of pinkeye cases.
If pinkeye is suspected, 5-8 swabs from acutely infected calves should be collected and submitted to the lab. Culture testing can differentiate and identify Moraxella bovis and Moraxella bovoculi and allow for antimicrobial susceptibility testing. Isolates can be preserved for autogenous vaccines. PCR-based molecular testing is used for agents like Mycoplasma bovoculi and IBR virus.
Two antimicrobials are labeled for treatment of pinkeye—oxytetracycline and tulathromycin—and prompt treatment is necessary for rapid resolution. If you have any questions, please email Dr. Dustin Loy.
Highest number of tularemia cases in 25 years
The Veterinary Diagnostic Center diagnosed tularemia in five cats during 2015. Four were from Nebraska (one southeastern, one central, two Lincoln area) and one was from northwest Iowa. Human cases in Nebraska were also elevated, with 18 diagnosed in 2015, the highest number in 25 years.
All animals were submitted with the clinical history of either acute septicemia, dyspnea, elevated temperature, oral ulceration, lymphadenopathy or icterus. Necropsies were performed either by the referring veterinarian or a pathologist at the VDC. Gross lesions in all animals were similar and consisted of a multifocal necrotizing hepatitis, lymphadenitis and splenitis. Francisella tularensis was isolated from the spleen and mesenteric lymph node from four of the cats.
Tularemia in a cat. Note the multifocal necrotizing hepatitis, splenitis and mesenteric lymphadenitis (arrows).Francisella tularensis is a zoonotic pathogen capable of infecting a wide range of domestic animals, wildlife, reptiles, birds and humans. Important reservoirs of infection are small rodents such as field mice, voles and lagomorphs including cottontail and jackrabbits. Vectors are deer flies, horse flies and ticks including the American dog tic (Dermacentor variabilis), the wood tick (Dermacentor andersoni), and the lone star tick (Amblyomma americanum). All of the abovementioned ticks are found in Nebraska.
Infection may occur via aerosol, direct contact, ingestion of the contaminated carcasses or water, or arthropod bites. Sheep are the most common domestic species to become infected, but infection has been reported in dogs, cats, pigs and horses. Cattle appear to be fairly resistant. Most wild carnivores such as bears, coyotes and foxes are fairly resistant to disease but have been reported to have developed antibodies against F. tularensis. Deer have been documented to carry the organism in their tonsils. Cats are particularly vulnerable to infection due to their predatory nature and propensity to ingest wild prey.
Tularemia should be suspected in cats exhibiting acute lymphadenopathy, malaise, oral ulceration, high fever and recent access to the outdoors. Diagnosis can be made by culturing liver, spleen and lymph node. Cultures of lymph node aspirated from live animals with lymphadenopathy are often successful in recovering the organism. The infectious dose of F. tularensis is very low (1-10 organisms); therefore, caution and proper personal protection equipment should be used in suspected cases.
Bovine respiratory disease PCR
Bovine Respiratory Disease (BRD) is one of the most common and costly diseases affecting beef cattle today. It accounts for over $1 billion in annual losses to the U.S. cattle industry, with preventative and treatment costs representing more than $3 million of that. In Nebraska and throughout the Midwest, the impact of BRD related deaths is significant.
To aid in the diagnosis of this costly disease, the UNL Veterinary Diagnostic Center is now offering BRD Multiplex Real Time PCR assays to screen for the bacterial and viral pathogens that are causative agents of the disease.
The BRD Multiplex Real Time PCR offers screening for the bacterial pathogens: Mannheimia haemolytica, Pasteurella multocida, Histophilus somni and Mycoplasma bovis, and the viral diseases: Bovine Viral Diarrhea (BVD), Infectious Bovine Rhinotracheitis (IBR), Bovine Respiratory Syncytial Virus (BRSV) and Bovine Coronavirus (BCV). The assays can be performed on lung tissues, tracheal washes, nasal swabs or deep nasopharyngeal swabs.
Benefits of PCR-based testing:
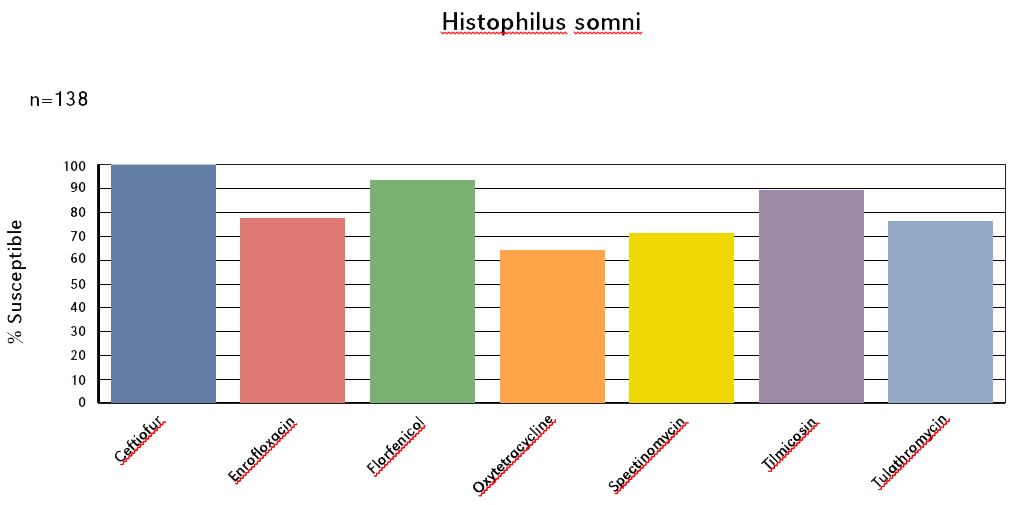
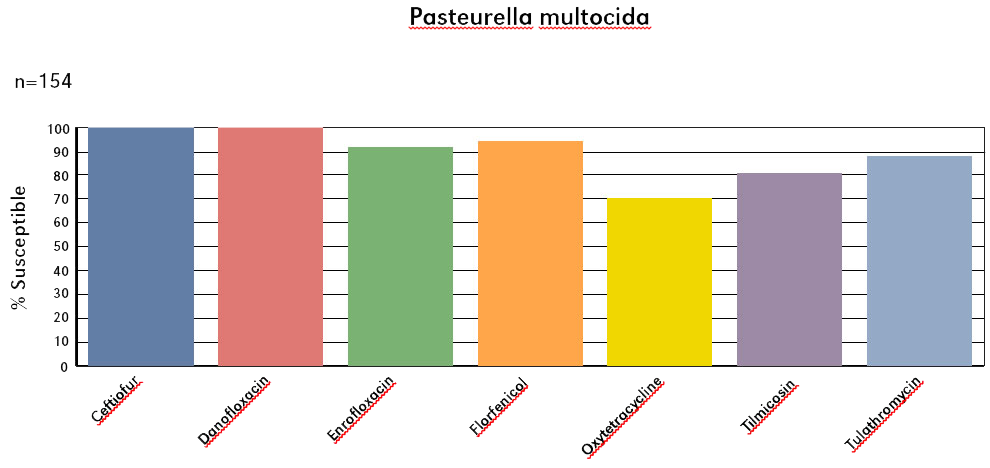
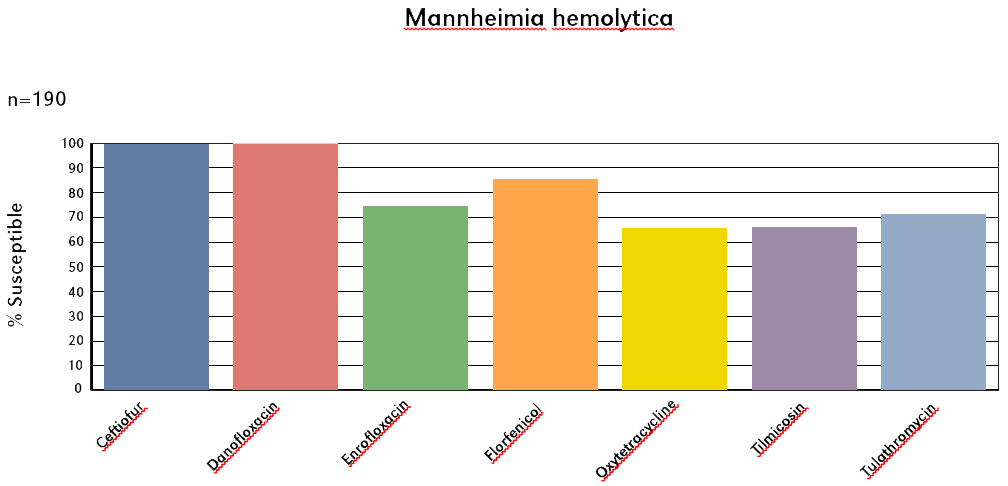
Ability to detect BRD related pathogens, especially bacterial agents within diagnostic samples that have been contaminated/mishandled, have undergone autolysis, and/or have been previously treated with antibiotics which may inhibit the recovery of these organisms on culture. A bacterial culture will be run in conjunction with the PCR in order to provide clients with susceptibility information on the isolates if needed (additional cost). In the instance where a pathogen comes up positive on PCR but the isolate was not viable, a percent susceptibility graph for each of the three bacterial pathogens is provided below.
Ability to offer a faster turnaround time and provide a more sensitive test method.
Please contact the laboratory if you have questions or need sampling supplies.
BRD Antimicrobial Susceptibility. MIC Interpretive criteria are based on CLSI guidelines VET01S 2015 for bovine respiratory pathogens.
Xylitol toxicosis in dogs
By Dr. Michael P. Carlson
Xylitol is a sugar substitute that is safe when ingested by humans but potentially toxic if ingested by dogs (Dunayer, 2006). It is used commercially as a low-calorie substitute for traditional sugars in foods and medicines, and dental products (Ravella S. R., Gallagher, Fish, & Prakasham, 2012). Consequently, dogs are usually exposed to xylitol accidently upon ingestion of a xylitol-containing product intended for use by humans.
The purpose of this article is to provide veterinarians with information about xylitol toxicosis in dogs, including mechanism of action, treatment and sources of exposure.
Effects in dogs Ingestion of xylitol by dogs produces an acute hypoglycemia (Dunayer, 2004; Dunayer & Gwaltney-Brant, 2006). The hypoglycemia seems to be due to direct stimulation of insulin secretion by xylitol acting on the pancreatic islet cells (Kuzuya & Kanazawa, 1969). Stimulation of insulin release by xylitol does not happen in humans.
Xylitol exposure at higher doses in dogs has been associated with hepatic necrosis and failure (Dunayer & Gwaltney-Brant, 2006; Dunayer, 2006). The hepatotoxic mechanism of action is unknown. Dunayer and Gwaltney-Brant propose two possibilities: prolonged hepatocytic ATP depletion or reactive oxygen species production as the result of hepatic xylitol metabolism.
Coagulopathy is a sequel to acute hepatic failure due to the cessation of hepatic clotting factor production.
Ingestion of xylitol by dogs at a dosage greater than 0.1 g xylitol/kg body weight can cause an acute, life-threatening hypoglycemia within 10-15 minutes (Dunayer, 2006; Pet Poison Helpline). Ingestion at doses greater than 0.5 g/kg can cause acute hepatic necrosis and failure (Dunayer & Gwaltney-Brant, 2006; Pet Poison Helpline). Estimating exposure is discussed later in this article.
Clinical signs Clinical signs include (Pet Poison Helpline):
Weakness
Lethargy
Collapse
Vomiting
Tremoring
Seizures
Jaundice
Malaise
Black tarry stool
Coma
Death
Clinical pathology, post-mortem and histological findings Common clinicopathology findings may include (Dunayer & Gwaltney-Brant, 2006):
Elevated liver enzymes in the serum
Hyperbilirubinemia
Hypoglycemia
Hyperphosphatemia
Prolonged coagulation times
Thrombocytopenia
Post-mortem lesions may include (Dunayer & Gwaltney-Brant, 2006):
Subcutaneous and visceral ecchymotic hemorrhages
Hemomediastinum
Hemoperitoneum
Pulmonary congestion
Edema
Icterus
Widespread hemorrhage in various places such as the kidneys, stomach, small intestine, pancreas, myocardium and lymph nodes
Histological findings may include (Dunayer & Gwaltney-Brant, 2006):
Acute periacinar and midzonal hepatic necrosis with periportal vacuolar degeneration
Subacute neutrophilic and lymphhoplasmacytic cholangiohepatitis with mild biliary hyperplasia
Differential diagnoses (Dunayer, 2006):
Parenteral insulin overdose
Oral hypoglycemic drugs such as glipizide or glyburide
Juvenile hypoglycemia
Hunting dog hypoglycemia
Pancreatic beta-cell tumor (insulinoma)
Idiopathic causes
Acute hepatopathy due to ingestion of acetaminophen, aflatoxins, Amanita phalloides and similar hepatotoxic mushrooms, blue-green algae, iron and sago palms (Cycas species)
Treatment of xylitol toxicosis (Dunayer, 2006) Minimize absorption. Emesis should be induced only if the animal is asymptomatic. Activated charcoal is not likely to beneficial.
If exposure dosage is estimated to be between 0.1 and 0.5 g/kg of xylitol, hospitalize the victim. Obtain baseline serum liver enzyme levels, coagulation time, and glucose, potassium, phosphorus and total bilirubin concentrations in serum. Monitor blood glucose concentrations every hour or two for at least 12 hours, and recheck the other tests every 24 hours for at least 72 hours. If hypoglycemia develops, administer a 1- to 2-ml/kg bolus of 25% dextrose intravenously followed by intravenous fluids containing 2.5% to 5% dextrose in order to maintain normal glucose concentrations. Correct severe hypokalemia (< 2.5 mEq/L) by adding potassium to the fluids. Treatment may be needed for 12 to 24 hours or until glucose concentrations can be maintained without supplemental dextrose.
If exposure dosage is estimated to be > 0.5 g/kg, treat the patient as described above, but start the dextrose treatment immediately regardless if a hypoglycemia has occurred. N-acetylcysteine (140 to 280 mg/kg loading dose followed by 70 mg/kg intravenously or orally q.i.d.), S-adenosylmethionine (Denosyl— Nutramax; 17 to 20 mg/kg/day orally), silymarin (Marin [Silybin]—Nutramax; 20 to 50 mg/kg/day orally), or vitamin E (100 to 400 IU orally b.i.d.) may be administered to protect the liver, but efficacies of those drugs for xylitol toxicosis have not been established. Transfusions of plasma or blood or both may be used to treat any coagulopathy that develops.
Prognosis (Dunayer & Gwaltney-Brant, 2006) The prognosis for uncomplicated hypoglycemia is good, with prompt treatment.
Cases involving mild increases in serum liver enzyme activities usually resolve within a few days with supportive care.
Prognosis for cases with more severe increases in liver enzyme activities, hyperbilirubinemia, and coagulopathy is guarded to poor. Additionally, hyperphosphatemia appears to be a poor prognostic indicator.
Sources of xylitol exposure Dogs are usually exposed to xylitol when they accidentally consume a xylitol-containing product intended for use by humans.
Xylitol is added to various products for human use for several reasons (Ravella S. R. et al., 2012). It is used as a substitute sweetener in diet foods and foods made for diabetics. It also prevents tooth demineralization, and dental caries by inhibition of bacteria that cause tooth decay (Ravella S. R. et al., 2012). Ravella, et al., describe it as an "anticarcinogen," which implies that it can inhibit carcinogenesis. The basis of that claim is not provided.
It is classified by the U.S. FDA as a food additive permitted for direct addition to food for human consumption (21 CFR Section 172.395, 2015; 21 CFR Section 172.395, 2015). Its use under that provision is described in that section of the Code of Federal Regulations as follows: "Xylitol may be safely used in foods for special dietary uses, provided the amount used is not greater than that required to produce its intended effect."
Its presence in dental products is not as an active ingredient for the prevention of tooth decay; it has apparently has not been approved by the U.S. FDA as an active ingredient for such purposes (Anonymous, 2003). The presence of xylitol in dental products seems to be as a non-sugar sweetener.
Products containing xylitol Several websites identify specific products or product classes that contain xylitol. The ASPCA Animal Poison Control Center lists product classes (ASPCA). Other websites may be found upon searching the internet. For example, the Preventative Vet website lists xylitol-containing products by product class and manufacturer or distributer within product class (Nicholas).
Some peanut butters contain xylitol, although their prevalence in retail outlets might not be very extensive. Dog owners who coax their dogs to consume oral medications by placing the medications in peanut butter should ensure the peanut better used does not contain xylitol.
Does a specific product contain xylitol? Check the product label to learn if xylitol in present in the product. Declaration of xylitol if it is present in a product is required by the Federal Food, Drug, and Cosmetic (FD&C) Act, the Fair Packaging and Labeling (FP&L) Act, and the regulations published by the Food and Drug Administration under the provisions of those laws. However, declaration of the amount of xylitol that is present is voluntary.
Nutrition label declaration of xylitol content in a food product need not occur unless a claim is made on the label or in labeling about sugar alcohol or sugars when sugar alcohols are present in the food. (21 CFR Section 101.9(c)(6)(iii), 2016). If it is declared and present in the food product at less than one gram, nutrition labelling regulations allow either of the following phrases on the nutrition label: "Contains less than 1 gram" or "less than 1 gram." If the serving contains less than 0.5 gram xylitol, the xylitol content may be expressed as zero.
Xylitol content is not included in the total carbohydrate declarations on a nutritional label of food products (21 CFR Section 101.9, 2016). Total carbohydrate includes sugars (monosaccharides and disaccharides), complex carbohydrates and fiber.
Estimation of extent of exposure If xylitol content is declared on the product labeling, exposure dose is more easily estimated.
If it is not declared, it is difficult to predict what amount might be present because xylitol content can vary, even between similar products. For example, xylitol content in some chewing gums is reported to range between 0.7 and 1.0 g per piece (Anonymous). Even so, an internet search for xylitol content in similar products might help estimate a likely exposure.
Anonymous. (2003). Proposed rulemaking 21 CFR part 356 oral health care drug products for over-the-counter human use; Antigingivitis/Antiplaque drug products. Federal Register, (May 29), 32232-32287.
Dunayer, E. K. (2004). Hypoglycemia following canine ingestion of xylitol-containing gum. Veterinary and Human Toxicology, 46(3), 137.
Dunayer, E. K. (2006). New findings on the effects of xylitol ingestion in dogs. Veterinary Medicine, December, 791-797.
Dunayer, E. K., & Gwaltney-Brant, S. M. (2006). Acute hepatic failure and coagulopathy associated with xylitol ingestion in eight dogs. Journal of the American Veterinary Medical Association, 229(7), 1113-1117.
Kuzuya, T., & Kanazawa, Y. (1969). Studies on the mechanism of xylitol-induced insulin secretion in dogs. Diabetelologia, 5, 248-257.
Ravella S. R., Gallagher, J., Fish, S., & Prakasham, R. S. (2012). Overview on commercial production of xylitol, economic analysis and market trends. In S. S. da silva, & A. K. Chandel (Eds.), D-xylitol: Fermentative production, application and commercialization (pp. 291-306). Berlin Heidelberg: Springer-Verlag.
It will soon be that time of year when feces are flowing faster and there is more fluid than anyone likes to see in neonatal calves. This article reviews some points to keep in mind when collecting antemortem or postmortem samples from calves for submission to the Veterinary Diagnostic Center.
Live, untreated calves in the early stages of disease are the best candidates for arriving at an etiologic diagnosis; however, owner reluctance to sacrifice a calf usually precludes this option. Frequently, samples received at the VDC consist of sections of small and large intestine in various stages of decomposition which may display virtually a rainbow of colors. Calves from which the samples originated frequently have been treated with one or more antibiotics. When intestinal samples are submitted, the time between death and postmortem examination usually ranges between 3 and 12 hours. There may be legitimate reasons for collecting these types of samples, but conclusive results are not often derived from such samples.
Practitioners faced with the decision of what to submit might want to reflect on a few points before collecting samples. Given the power of molecular techniques such as PCR to detect tiny amounts of pathogens, a herd-level diagnosis can frequently be achieved by collecting several grams of feces that is representative of the clinical picture. The VDC runs a multiplex PCR panel that enables testing for the most common viruses, bacteria and parasites in one assay. Fecal specimens can be pooled together or run individually to determine the pathogens present. Additionally, these tests enable quantification of the amounts of each pathogen in the specimens using a cycle threshold, or Ct value, to assist in interpretation of diagnostic findings.
When submitting feces from calves with diarrhea, it is advisable to collect several grams (preferably 10 or more) of feces from at least three calves that have not been treated (especially when bacterial enteritis is suspected). Swabs DO NOT contain adequate material to ensure a uniform sample for PCR testing. Generally, a few days after infection occurs, concentration of the etiologic agent/s in feces may be too low for detection. Considering clinical signs may not appear for at least a day after infection, the window of opportunity for collecting a fecal sample with detectable amounts of the etiologic agent/s is relatively small. Usually the value of a fecal sample diminishes rapidly about 12-18 hours after initiation of clinical signs. Feces or distal large intestine contents are superior specimens compared to small intestinal contents. Remember, most coronavirus infections and coccidia infections occur primarily in the large intestine in cattle.
Common Pathogens In calves less than 4-5 days old Escherichia coli would be the primary differential followed by Clostridium perfringens type C. Gross lesions are rarely seen in cases of colibacillosis; however, bacterial colonization is observed histologically in the ileum. In Clostridial enteritis, the lesion is that of severe necrotic enteritis and is usually located in the proximal ileum and jejunum. Rotavirus may be implicated any time before 2-3 weeks of age but is more commonly seen in calves older than 4-5 days. Coronavirus can be encountered at nearly any age of the calf, but after a few weeks of age (as with rotavirus) it is generally not a severe problem. There is no gross or histologic distinction between the lesions caused in the small intestine by either rotavirus or coronavirus. Coronavirus does cause lesions of mucosal cryptitis in the colon, which rotavirus does not. Vaccine strains of rotavirus and coronavirus may be shed in feces but only sporadically and at a low concentration compared to virulent strains. Differentiation between vaccine and field strains cannot be made by conventional methods. Because of the protozoan life cycle, they should be considered in a differential diagnosis after 5 days of age. The most common protozoan encountered is Cryptosporidium parvum. Eimeria spp. are not commonly seen in calves less than 3 weeks old.
Less Common Pathogens Some of the less commonly encountered intestinal pathogens are Salmonella sp., bovine virus diarrhea (BVD) virus and bovine adenovirus. Salmonellosis is occasionally encountered but usually at an age of 2-3 weeks. However, recent outbreaks of Salmonella, including Salmonella serovar Dublin have been found in high risk or mixed source dairy calves. Often the lesion seen with salmonellosis is that of catarrhal or hemorrhagic enteritis and is usually confined to the ileum in the early stages, but can be seen in the jejunum and colon later in the disease. BVD may cause lesions similar to those seen in salmonellosis and coronavirus infection. Attaching and effacing E. coli can occasionally cause diarrhea in 2- to 4-week-old calves. These are frequently diagnosed by histopathological observation of the bacteria, combined with culture and PCR testing for the appropriate virulence factors.
While PCR testing of feces has replaced most of the old test methods, it is still important to collect intestinal segments from appropriate locations within the intestinal tract. At a minimum, a segment of ileum and colon should be submitted. Minimum samples for histopathology should include at least two nonadjacent sections each from the ileum and colon. Depending on the suspected disease, fresh and fixed segments from other regions of the intestinal tract are necessary. As noted above, autolytic changes greatly reduce the chances of an accurate diagnosis. Autolysis begins immediately after death and because of this fact it is important that samples be collected as soon as possible. Within minutes, epithelial cells begin to slough off the intestinal mucosa beginning at the tips of villi and are easily washed away during processing. When present, mucosal crypt and deeper lesions may still be visualized but the ability to evaluate villous length and changes in the epithelium at the distal end of villi is lost. Intestine segments should be opened before immersion in formalin and do not need to be any longer than one inch (an unopened segment of intestine immersed in fixative even from a euthanized animal will have autolytic changes in the mucosa). Sloughing of villous epithelium due to autolysis greatly hampers accurate histologic diagnosis of the most common enteric diseases. Lesions are seen grossly in the jejunum. Segments of Mesenteric lymph node and Peyer's patch are best for BVD virus identification. For bacterial culture, the ileum is preferred over jejunum unless obvious lesions are seen grossly in the jejunum. Segments of fresh small intestine and colon need not be longer than 6 to 8 inches. Diagnosis of Cryptosporidia parvum is either by identification of the organism histologically or acid-fast stained smears of intestinal contents. Coccidia are identified either on fecal floatation or by histology.
One of the best methods of prevention of calf diarrhea is by utilizing the Sandhills Calving System. Sometimes even the best management may realize outbreaks of diarrhea but with proper and timely sample submission a quick and accurate diagnosis can be made.
Pathogen
Age
Test
Specimen
E. coli (F5/K99)
2-5 days
PCR Panel/Culture
Feces
Cryptosporidium
≥ 5 days
PCR Panel/Acid Fast
Feces
Rotavirus
≥ 7 days
PCR Panel
Feces
Coronavirus
≥ 7 days
PCR Panel
Feces
C. perfringens
Histopath/Culture
Fixed/Fresh Intestine
Salmonella
2-12 weeks
PCR Panel/Culture
Feces
Eimeria (Coccidia)
≥ 2 weeks
Floatation
Feces
Coronavirus
≥ 7 days
PCR Panel
Feces
Questions about PCR Calf Panel Testing? Contact: Dr. J. Dustin Loy, DVM, PhD, DACVM Veterinary Microbiologist Phone: 402-472-1434 Email: jdloy@unl.edu
Good sample handling minimizes errors
Handling practices that may create errors:
Caps on tubes were not completely snapped on and the samples leaked in the bag. Tubes were labeled with a marker and several of the IDs wiped off. Tubes arrived covered with fecal matter.
Samples are mislabeled. The ID on the sample does not match the ID on the submission form.
Fecal samples sent in gloves leaked inside the Ziplock bag.
The ID on the sample is completely or partially wiped off. If a Sharpie is used and the container gets wet, the ink will wipe off.
Example of a nonsterile container used to submit a bacterial culture sample. The cup could easily break, and the Press'n Seal used as a lid can easily come off, allowing the sample to leak.
The ID is not listed on the submission form.
The ID on the submission form and/or sample is difficult to read.
Samples leak during transit and the contents mix together. Formalin or other liquids in Whirl-Pak bags or Ziploc baggies rarely stay contained in the bag during shipment. If one of these bags must be used, be sure to double or triple bag to avoid spills. If using a Whirl-Pak bag, be sure to properly close the top to help prevent leakage. Whirl-Pak provides instructions for proper closure on their website.
Fecal samples are submitted in baggies or gloves. It is very difficult to remove the feces without contaminating other samples and supplies.
Solutions to reduce errors:
Always list the ID on the submission form. An Excel spreadsheet can be used and e-mailed to the VDC. The IDs can be directly uploaded into our system, eliminating the possibility of data entry errors.
Double check that the ID on the submission form matches the one on the sample. VDC submission forms can be found on our website.
Use a marker that won't wipe off or a label that will not come off. Clean off any fecal matter, blood, etc., before labeling the tube.
Write as legibly as possible.
Rack the samples before sending them, preferably in the order on your submission form. The VDC will provide divided boxes upon request.
Submit samples in tubes or jars. The VDC will supply tubes or jars to your lab upon request.
Winter shipping tips
Preventing frozen biopsy samples Now that cold weather has arrived, it's time to add ethanol to biopsy samples to prevent freezing in-transit.
Adding 1 part ethanol to 9 parts formalin during the winter is sufficient to prevent freeze-thaw artifacts, which could hinder the pathologist's interpretation of the biopsy sample. Ethanol can be purchased at any hardware store as "denatured alcohol" and added to your formalin jars. Clients who receive biopsy mailers from the VDC during the winter months will already have ethanol added. This is indicated by a sticker on top of the jar that says "10% ethanol added."
Feel free to contact the VDC with any questions.
Shipping trichomonas samples With breeding season just around the corner, we want to remind you of the importance of properly shipping your trichomonas tubes and pouches during the winter months.
If you are sending trichomonas samples that have not been incubated prior to shipment, adding warm packs and shipping in a Styrofoam cooler will help ensure proper temperature is maintained. If you don't have warm packs, microwaving a cold pack is an acceptable alternative. Make sure warm packs avoid direct contact with samples. We also suggest avoiding weekend shipments due to the possibility of packages sitting at sites where temperature is not regulated.
Other shipping tips During the winter months there is always the chance of severe weather events affecting the delivery of shipments. When shipping tissues, adding adequate cool packs and using coolers is a good way to help ensure samples are kept cold in the event of prolonged shipping times.
Although it is infrequent, there are times when packages do not reach the VDC in the time specified by the shipper. If you have a time sensitive shipment and want to verify that we received the package, please email us the tracking number and contact information. We will confirm the receipt of your samples when we receive them.
VDC construction update
Architectural drawing of the new Veterinary Diagnostic CenterVeterinary Diagnostic Center under construction. The photograph is from the northwest looking southeast. The arrow indicates the front entrance.
In late June construction of the Veterinary Diagnostic Center began with ground site preparation, utility installation and excavation for the two-story building. Since then construction as progressed steadily. The outer walls and many of the interior supporting walls have been erected, and ground floor slabs have been poured. Framing of the exterior walls is underway.
It is expected that the exterior walls of the building will be completed shortly which will allow for enclosure and heating of the work space. Work crews will then focus on the interior mechanical, plumbing and electrical work.
The completion date has been moved back a month to early January 2017 due to weather related delays. The potential of unexpected delays was taken into consideration in the initial building schedule. All in all, progress is on schedule and occupation of the building is expected to begin by mid to late February 2017.